

At first go, it is hard to notice 26-year-old Beena Devi lying on the bed of gynaecology ward of Shri Mahant Indiresh Hospital, a private hospital in Dehradun. Reduced to 45-kg, she is only bones covered with a thin, pale layer of skin and hollow eyes popping out of eye sockets. A urine bag hangs from her side while her left hand is pockmarked with intravenous injections to feed her fluids and medicines. Flesh on her body has shrunk so much that the nurse has to daily struggle to find veins under the skin of her wrist to administer her medicine and glucose.
A couple of weeks back, on June 21, Beena, a resident of Kaprada village in Chinyalisaur block of Uttarkashi district, underwent hysterectomy — removal of uterus — at the district hospital Uttarkashi. More than three weeks later, she was still bleeding profusely, now lying on the bed of a private hospital in the state capital.
“After the surgery, my condition kept worsening, so on July 11 my husband rushed me to a hospital in Dehradun. My stitches have punctured and I am in great pain,” Beena told last month to Gaon Connection while wreathing in pain on the hospital bed. “I feel nauseated all the time and have lost my appetite,” she added.
Beena has three young children aged seven, five and three years. She isn’t sure if she will survive and watch her kids grow.
")
Beena undergoing treatment in a private hospital in Dehradun after her uterus was removed in the district hospital in Uttarkashi (Photo: Megha Prakash)
Beena’s case exposes the poor rural healthcare infrastructure and services in the hill state.
It was on June 20, a day before Beena’s ill-fated surgery, when all hell broke loose. Sunil Rana, Beena’s husband, got a distressed phone call from his parents. Rana, who works as a cook in Rudrapur, an industrial town bordering hills of Kumaon about 500 kilometres (kms) away from his village in Uttarkashi, was informed his wife was seriously ill and had to be urgently taken to the district hospital at Uttarkashi, over 70-80 kms away from Kaprada village. Before he could understand anything, the phone disconnected. Rana immediately left for home in a state transport bus, which took 12 hours to reach his village.
But, the horror had just begun. There was no vehicle to transport Beena to the district hospital in Uttarkashi. “I called the hill ambulance number – 108 – twice. The person at the other end of the phone call kept asking to share location, but in spite of providing all the information, no ambulance came,” Rana told Gaon Connection.
The public transport system in hilly areas is paralysed. The local shared taxis, the only means of commute for villagers in the hills, are limited and not very frequent, said Rana. “I borrowed Rs 5,000 from neighbours and relatives and rented a private car. By the time we reached the district hospital Uttarkashi, it was already 7 pm. A preliminary examination was done on my wife and we were told to wait until the next morning,” he added.
Next morning, when Beena’s abdominal pain and bleeding did not subside, the on-duty senior surgeon advised immediate surgery to remove her uterus. Post hysterectomy, her condition worsened. Beena’s haemoglobin dropped to 6.8 grams per decilitre (a healthy adult woman’s haemoglobin should be 12.0- 15.5 grams per decilitre) and she remained unconscious for 12 hours.
Her uterus, surgically removed from her body, was handed over to her husband wrapped in a newspaper. He was assured his wife would recover soon.
More than a week later when things did not improve, Rana decided to shift his wife to a hospital in Dehradun, much against the wishes of the district hospital where his wife was operated. By then, the medical expenses had already crossed Rs 35,000.
On July 11, Beena was brought to a private hospital in Dehradun, where she underwent treatment. She was finally discharged on July 31 after her condition stabilized. “Beena was brought in a distressed state. She has now been discharged with one month medication,” said a doctor of Shri Mahant Indiresh Hospital on condition of anonymity.
Beena’s case isn’t a one-off case of poor health services in rural Uttarakhand. The public health system in Garhwal and Kumaon hill regions of Uttarakhand is in dismal state.
")
Suman Devi who works as anganwadi head in Dwara coordinates monitoring of expecting ladies in the village with ASHA and ANM workers at the PHC. (Photo: Megha Prakash)
“Most health centres in rural areas have no basic screening facilities, such as X-ray machine, pathology laboratory or ultrasound facility. This makes it extremely difficult for doctors to diagnose and treat patients. Therefore, villagers have to be referred to the nearest district hospital in Kotdwar,” said Rahul Lakhera, a pharmacist employed at government-run state-allopathic dispensary (SAD) in village Kinsur of Dwarikhaal block in Pauri Garhwal. According to him, there is a shortfall of doctors in rural areas, but even if they are deployed in remote areas, unless medical facilities are made available, doctors can’t do much.”Besides, many of these public health centres have modern buildings, but have poor facilities,” said Lakhera.
Officially, each block of the state has one primary health centre (PHC), sub-centre, additional primary health centre. But, they lack the requisite infrastructure. Last year, to fill vacant positions, 446 doctors were appointed, but grade IV positions are still lying vacant.
“There is no ambulance facility, no delivery ward and no lady doctor to attend emergencies in the PHC at Dwara Samoli village of Raipur block. We are dependent on the CHC [community health centre] in Raipur, which is eight kilometre away, or the Doon Hospital,” said Subhash Chandra Negi, a local tea-shop owner in Dwara Samoli village.
")
The PHC building in village Dwara Samoli of block Raipur, district Dehradun, is pateint unfriendly (Photo: Megha Prakash)
Health in doldrums
In its July 11 report, The Pioneer highlighted shortage of health specialists in the state. It noted the state health services did not have a single specialist of cardiology in the entire state and had only 393 specialist doctors in its ranks out of sanctioned posts of 1,234.
Mountainous districts like Pauri, Tehri, Bageshwar, Uttarkashi and Chamoli are more affected by the shortage of doctors. There are no orthopaedic surgeons in Tehri and Bageshwar districts and not even a single ENT surgeon in Tehri, Chamoli and Bageshwar districts.
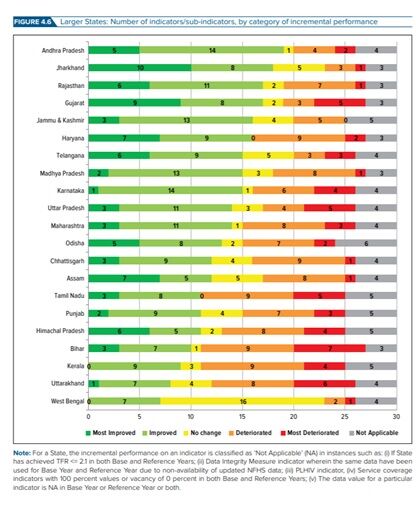
This situation is rampant throughout the hill state and to an extent corroborates with the recent findings published in the second edition of Healthy States Progressive India Report of the Niti Aayog released in June this year.
According to NITI Aayog’s Health Index 2019, Uttarakhand fared poorly because of high rates of neonatal and under-five mortality, low stability of key administrative positions at district levels, a 30-percentage-point reduction in functionality of primary health centres performing specified number of C-sections per year, and National Health Mission fund transfer delays (see graphic: Slipping away).
Source: NITI Aayog Report 2019
The NITI Aayog 2019 report notes that the state’s neonatal mortality rate [neonates are newborns from 0-6 months age] has increased from 28 deaths per 1,000 live births to 30, and its under-five mortality rate (U5MR) has increased from 38 to 41.
Meanwhile, the National Family Health Survey 2015-16 (NFHS-4) has also reported poor health indicators in Uttarakhand. It noted infant mortality rate (IMR) and U5MR of 44 and 49 per 1000 live births in the state, respectively. This is way behind the national average statistics.
And, poor rural health infrastructure is a major contributing factor in low ranking of the state in the recent health index of NITI Aayog. For instance, residents of Chuna Mehedda village, located on a hill-top in Pauri district’s Dugadda block, don’t have a motorable road and the nearest PHC is seven kms away in Pokhal, a small market town.
") A private jeep follows track marks running through river Malan to village Chuna Mehedda in Dugadda block, Pauri Garhwal (Photo: Megha Prakash)
A private jeep follows track marks running through river Malan to village Chuna Mehedda in Dugadda block, Pauri Garhwal (Photo: Megha Prakash)
The sick villagers have no choice, but to depend on private jeeps which run through the gushing waters of river Malan to reach Pokhal PHC. During heavy downpour of monsoon, the river swells and for one month-and-a-half, the villagers of Chuna Mehedda are completely cut-off. “The sick are then carried on a stretcher or charpoy for an hour,” said Jagadish Kukreti, a resident of Chuna Mehedda.
“Sometimes women in labour or animal attack victims are tied to cots and taken to the nearest PHC, seven kilometres away, for medical aid. That is why several women prefer child birth at home than be transported on cots to the health centre, said Kukreti.
Officials in-charge of PHCs in the state claim they were trying to do their level best to provide health services to local people. “At our PHC, on an average we conduct 100-150 child deliveries per month. We also cater to 150-200 patients in our OPD on a daily basis. But, many PHCs in the state lack basic facilities, a fact which cannot be ignored,” said Shyam Vijay, in-charge of Pilkhi PHC in Bhilangana block in Tehri Garhwal. This PHC caters to over 200 villages.
")
A doctor attending to a villager at Pilkhi PHC (Photo: Shyam Vijay)
Research highlights poor health services
Last year, a scientific research study published in International Journal of Contemporary Pediatrics looked at neonatal mortality in the state. It evaluated the magnitude of post neonatal mortality [death of a newborn between 28 days and 1 year of age expressed per 1,000 live births] and its seasonal pattern at Hemawati Nandan Bahuguna Teaching Base Hospital, Srikot in Garhwal over a period of 10 years. This base hospital, about 150 kms from the state capital, serves people of four districts of Uttarakhand that include Tehri Garhwal, Rudraprayag, Chamoli and parts of Pauri Garhwal.
Researchers of this study reported an overall post neonatal mortality of 1.83 per cent, out of which the mortality amongst boys was 119 (54.34 per cent) and girls was 100 (45.66 per cent). Three most common causes of mortality, according to the study, were septicemia (27.40 per cent) followed by encephalitis (11.41 per cent), and protein energy malnutrition or underweight (9.58 per cent). Septicemia, also known as sepsis, is a life-threatening complication that can happen when bacteria from another infection enter the blood and spread throughout the body.
The researchers of 2018 study concluded that post neonatal deaths could be reduced by strengthening vaccination program, facilities at tertiary care centres and healthy dietary practices in the community. A tertiary referral hospital is a hospital that provides tertiary care, which is a level of health care obtained from specialists in a large hospital after referral from the providers of primary care and secondary care.
Poor design and inaccessible health centres
Apart from lack of health officials and poor screening facilities, several health centres in the state epitomise bad structural design and are inaccessible. For instance, to reach the Kinsur SAD in Dwarikhaal block of Pauri Garhwal, villagers have to walk for an hour, as it is located on an abandoned land off the village periphery. “That is why instead of visiting the nearest health centre, villagers prefer district hospitals, which adds to the burden of these district centres,” said Lakhera.
Similarly, the entrance to the health centre in Soda Saroli in Raipur block in Dehradun does not have clear passage or a walkway.
") Left: A Women and Child Health Facility at Maldevta in Raipur| Right: An obstructed entrance of PHC is Soda Saroli of Raipur block in Dehradun (Photos: Megha Prakash)
Left: A Women and Child Health Facility at Maldevta in Raipur| Right: An obstructed entrance of PHC is Soda Saroli of Raipur block in Dehradun (Photos: Megha Prakash)
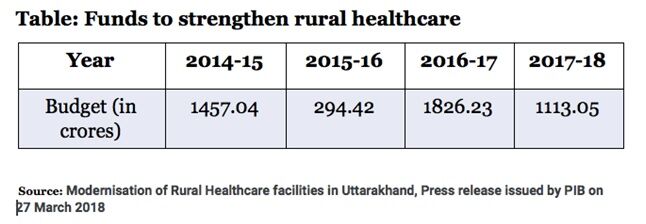
Under the State Implementation Plan (SIP) of National Health Mission, the Centre allocates budget for modernization, strengthening and new construction/renovation of rural healthcare facilities by the Centre. Between 2014 and 2018, Rs 4690.74 crore was allocated to build/renovate rural health centres in Uttarakhand (see table: Funds to strengthen rural healthcare). But, the situation in the field is far from satisfactory.
For instance, last year, researchers from Delhi-based Population Research Centre, Institute of Economic Growth, monitored & evaluated implementation of National Health Mission Programme in Kumaon’s two districts Naintal and Almora. In Nainital district, the researchers found the health infrastructure pertaining to neonatal health inadequate. At the Motahaldu PHC, for example, there was no radiant warmer [a body warming device to provide heat to the body of the baby and limit the metabolism rate.] in place. Also, sterilised delivery sets and neonatal resuscitation kit were unavailable.
Based on their visits to B.D Pandey Female Hospital, CHC Bhowali, PHC Motahaldu, sub-centre (SC) Bhowali and sub-centre Gangapur Kobarwal in Nainital district, the team noted: “The district has 8 CHCs, 15 PHCs and 136 SCs. With respect to transport, 13 ambulances and 9 referral transport are available. No mobile medical units are available in the district. All the visited health care facilities such as District Hospitals (DHs), Community Health Centres (CHCs), Primary Health Centres (PHCs) and Sub-Centres (SCs) are running in government buildings. However, the infrastructure in the health facility premises was not proper.”
It went on to record that “location of certain facilities (SC Gangapur Kobarwal, for instance) is such that approaching the facility is not feasible conveniently. Better location of the health centre is of the need.” Researchers also noted that staff quarters were not available in the PHC Motahaldu. Further, there were vacancies for medical officers, anaesthetists, staff nurses, pharmacist, data entry operators, accountants and fourth-class employees in the district.
Similar findings were reported in Almora district of the state, which has s even CHCs, 26 PHCs and 203 SCs.
The state government claims it is trying to address the issue of poor rural health infrastructure. To fill vacant posts in rural areas, it brought in the Transfer Act 2017.
As per this Act, the state government introduced subsidised MBBS courses. The beneficiaries were asked to sign a bond mandating a compulsory five-year service in ‘durgam’ and ‘sugam’ areas after completing the degree, failing which the beneficiary shall be liable to pay the government Rs 1 crore as penalty. An MoU with medical school in Haldwani was signed.
This move faced opposition from the Uttarakhand Medical Services Association because of lack of residential, medical testing and basic living facilities in rural areas of the state.
To overcome the gaps in service delivery, in 2013 the government then decided to implement PPP-based projects and handed over five government hospitals to private parties.
Tehri district is leading in PPP-based health projects, where the district hospital and the Combined Health Centres (CHCs) are being run by private companies. CHCs in Dehradun, Devprayag and Bageshwar have been privatised. Meanwhile, the conversion of CHCs in Almora and Nainital districts to PPP mode is also under consideration.
However, all is not well with this privatisation of health facilities in the state. Recently, the local administration expressed discontent on the functioning of district hospital in Tehri managed by Dehradun-based Jolly Grant Himalayan Hospital under the PPP mode. Recently, on July 18, the new district administrator, V Shanmugan on a surprise visit to the district hospital in Bauradi, Tehri noted the dismal state of hospital. During his visit, he observed that the technicians returned patients after performing mere 20 ultrasounds in a day. The nebulizer in the emergency ward was also found not functional.
Read Also: Rural India ditches govt hospitals, opts for private doctors: Gaon Connection Survey
Read Also: Deprived of ambulances, charpoy and boats are the only means of transport during a medical emergency

















